IMPLA Multi Unit Concept
Treatment schedule planning
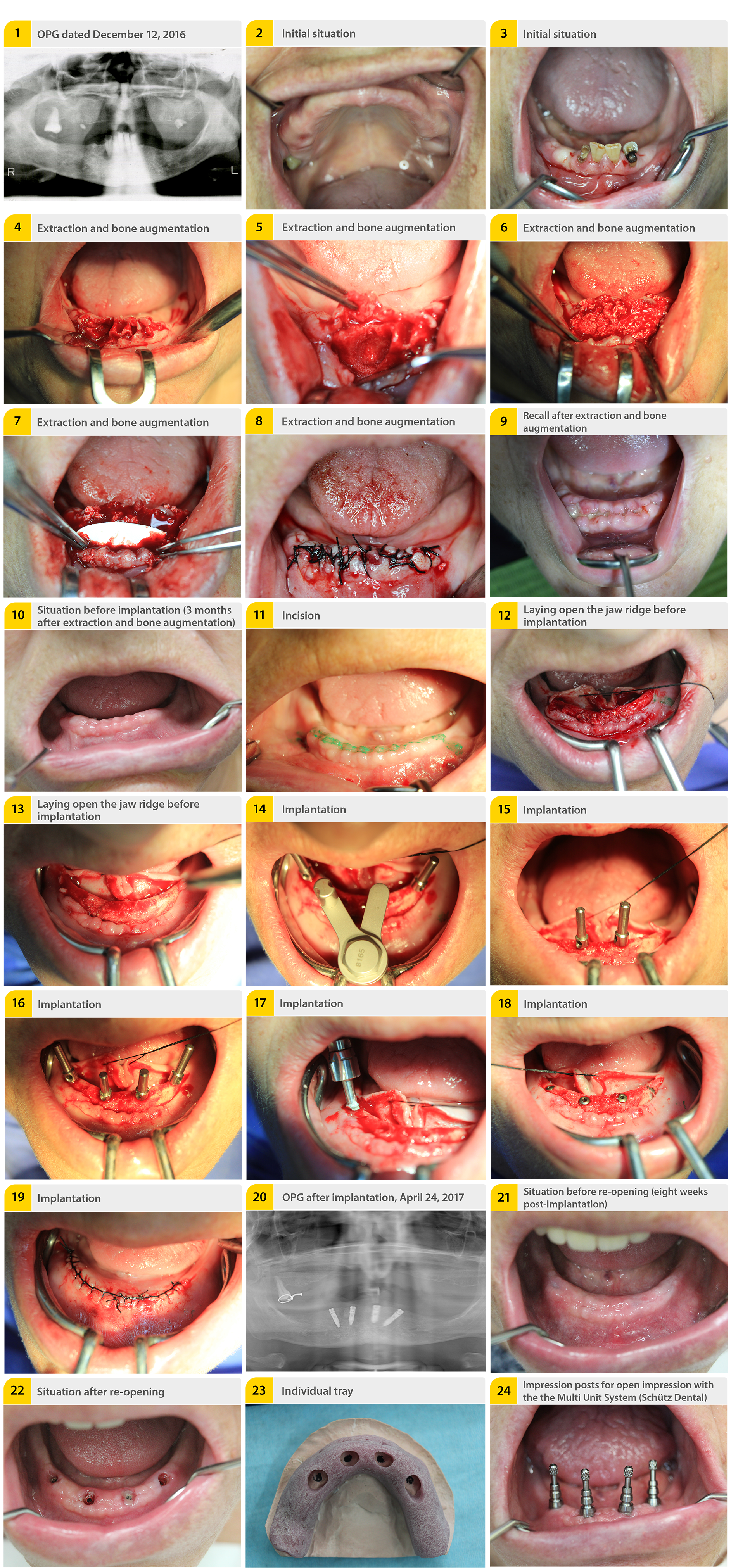
Considering the reduced bone supply and the deficient bone height especially in the third quadrant, we planned the placement of four interforaminal implants in accordance with the Multi Unit Concept. The distal implants were planned with an angle of 30° (fig. 1: OPG, fig. 2 and fig. 3: Initial situation). The implants are placed interforaminally and the distal implants were inclined by 25°-35° in distal direction. This procedure provides an extension of the support polygon. The position of the distal implant is mesial and the implant exit point is above or distal to the mental foramen. Consequently, there is normally sufficient bone height even for longer implants with an accordingly higher stability.
First surgery: Extraction and augmentation
We started the treatment end of January 2017. The initial step was to extract the remaining teeth in the mandible as well as the remaining roots in both jaws. Next, we started an extensive augmentation at the place of the bone defect and of the missing bone lamella (area of lower right cuspid) with autogenous bone and xenogeneic material. The augmentation was covered by an absorbable collagen membrane. (extraction and augmentation, fig. 3-8). 10 days post-surgery, the sutures were removed (fig. 9).
Second surgery: Implantation
After a healing phase of approximately three months (fig. 10), the implants were inserted. First, we made a crestal incision from the area of the lower right cuspid to the area of the lower left 1st bicuspid, with distal relief incisions (fig. 11). The jaw ridge and the mental foramen were layed open. The bone graft was completely ossified (fig. 12 & 13). The implantation site for four implants was prepared in accordance with the drill protocol of the manufacturer (Schütz Dental, Rosbach/Germany). The distal implants were inclined by approximately 30° and they passed by the mental foramen mesially (fig. 14-16). After the insertion of the implants (fig. 17) and after covering them with healing caps (fig. 18), we closed the wound saliva-proof with a 3-0 silk suture (Schütz Dental, Rosbach/Germany) (fig. 19). The panoramic radiograph shows the situation directly post-implantation (fig. 20).
Re-Opening
8 weeks post-implantation we re-opened the implants (fig. 21 & 22). Next, we produced an individual tray for an impression (fig. 23) and took an impression with help of the Multi Unit impression posts and abutments (Schütz Dental, Rosbach/Germany) (fig. 24). After transferring the situation to the model (fig. 25), an acrylic pattern was used to create a transfer key (fig. 26-28). It was tried in (fig. 29) and the abutments were fixed (fig. 30 & 31).
Bar Construction
The dental lab (Bisswerk, Aachen/Germany) produced the bar construction and the secondary framework (fig. 32 & 33). This was tried in again in clinical context (fig. 34). The fit of the bar construction was verified with the Sheffield test (fig. 35).
Denture
Next, the dental lab (Bisswerk, Aachen/Germany) created the denture (fig. 36-39). Finally, the position of the implants and of the bar construction was checked radiologically in an OPG (fig. 40). The restoration was finalized in September of 2017. During a subsequent recall appointment, the denture and the bar construction were checked and cleaned.
Discussion
The concept of the distally angulated implants goes back to Kerkmanov, 1990 [Kerkmanov et al., 2000], but was only established at the beginning of the 21st century with the „All-on-4“ concept of Paolo Malo [Malo et al., 2003, 2005, 2006, 2007, Kathami & Smith, 2008]. This treatment facilitates providing a restoration for an edentulous jaw without complex augmentation, even in one of the many cases like this one, where there is limited vertical bone available in the posterior region of the mandible. In this case, the remaining bone height was not sufficient for an insertion of standard length implants in distal position from the mental foramen. Therefore, we decided on an interforaminal implantation. To extend the prosthetic support polygon, the distal implants were inclined by ca. 25-35° in distal direction, in accordance with the above mentioned concept.
The preceding augmentation of the bone defect after extraction in the area of the lower right cuspid was carried out with xenogeneic bone substitute and a collagen membrane in line with the „socket preservation“ [Troiano et al., 2017, Vignoletti et al., 2012]. The augmentation was extended to the other extraction sockets to optimize the situation for the planned implantation. The extraction as well as the bone augmentation and implant surgeries were free of complications and the wound healing was completely uneventful. The prosthetics were manufactured in cooperation with the dental lab Bisswerk in Aachen/Germany. With the prefabricated parts of the Multi Unit System (Schütz Dental, Rosbach/Germany), an individualization of the abutments could be foregone for an easier and quicker completion. The Multi Unit System was used in combination with cylindrical implants (Schütz Dental, Rosbach/Germany), as these implants offer the greatest primary stability due to their self-tapping thread and the cylindrical external geometry.
As a complete system, the wide selection of abutments as well as auxiliary parts for closed and open impressions offers easy and clear options for quick treatment concepts with angulated implants in the upper and lower jaw. Considering progress and the desire for easy-to-implement and economical solutions, using this system is the logical next step.
Especially for concepts of „everything from one source“, the use of the Schütz Dental Multi Unit System produces excellent results.

Literature
1. Maló P, Rangert B, de Araújo Nobre M. „All-on-Four“ immediate-function concept with Brånemark System implants for completely edentulous mandibles: A retrospective clinical study. Clin Implant Dent Relat Res 2003; 5 (Suppl 1): 2-9.
2. Maló P, Rangert B, de Araújo Nobre M. All-on-4 immediate-function concept with Brånemark System implants for completely edentulous maxillae: A 1-year retrospective clinical study. Clin Implant Dent Relat Res 2005; 7 (Suppl 1): S88-94.
3. Maló P, de Araújo Nobre M, Petersson U, Wigren S. A pilot study of complete edentulous rehabilitation with immediate function using a new implant design: Case series. Clin Implant Dent Relat Res 2006; 8:223-232
4. Maló P, de Araújo Nobre M, Lopes A. The use of computer-guided flapless implant surgery and 4 implants placed in immediate function to support a fixed denture: Preliminary results after a mean follow-up period of 13 months. J Prosthet Dent 2007; 97(suppl):S26-S34.
5. Krekmanov L, Kahn M, Rangert B, Lindström H. Tilting of posterior mandibular and maxillary implants of improved prosthesis support. Int J Oral Maxillofac Implants 2000; 15: 405-414
6. Troiano G, Zhurakivska K, Lo Muzio L, Laino L, Cicciù M, Lo Russo L. Combination of Bone Graft and Resorbable Membrane for Alveolar Ridge Preservation: a Systematic Review, Metaanalysis and Trial Sequential Analysis. J Periodontol. 2017 Sep 12:1-17. doi: 10.1902/ jop.2017.170241.
7. Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin Oral Implants Res. 2012 Feb;23 Suppl 5:22-38. doi: 10.1111/j.1600- 0501.2011.02331.x.
8. Khatami AH, Smith CR. “All-on-Four” immediate function concept and clinical report of treatment of an edentulous mandible with a fixed complete denture and milled titanium framework. J Prosthodontics 2008;17(1):47-51
Download this case study as PDF file:
Read now!Please note: This case study is not an instruction leaflet. Please adhere to the instructions provided with the material and/or equipment. The responsibility for the treatment remains with the attending dentist.

Tactile scans ... are worth the effort!

Bleaching with "Bleach’n Smile“

Case study: Cervical Fillings with PrimeBond7 and Capo Slow Flow
